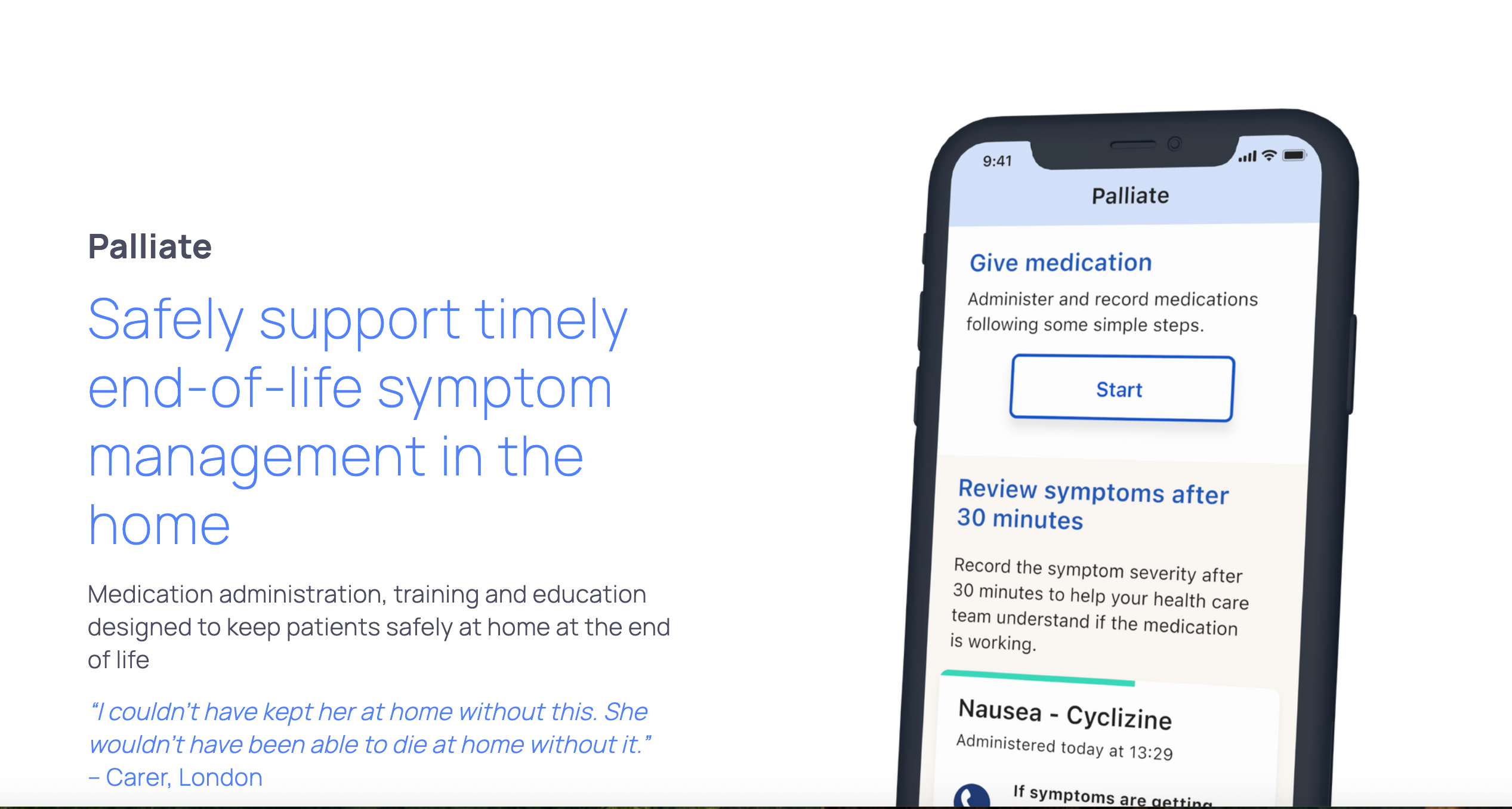
In our fragile final hours, comfort often depends on something surprisingly practical, the timely access to symptom-relief medication. When community nurses are delayed, pain rises, breathlessness grows, families panic, and the moment becomes harder than it needs to be. At the Helix Centre, part of Imperial College London, researchers are asking a simple but radical question, ‘What if families felt ready?’ What if trusted partners, children, or close friends could be safely trained to give that relief themselves? This is the heart of Palliate, a project led by Dr Sunkersing and funded by the Oak Foundation, rooted in lived experience and quietly reshaping what compassionate end-of-life care at home could look like.
“A lot of people want to die at home, but timely symptom relief can be difficult… especially when a nurse has to travel long distances.”
Why This Innovation Matters
The UK has around 6.2 million carers, and half a million support someone with a terminal illness. Many already manage complex daily tasks, yet they are rarely offered structured training for moments where help matters most. And the need is clear. As Dr Sunkersing explains, “A lot of people want to die at home, but timely symptom relief can be difficult… especially when a nurse has to travel long distances.”
He adds that even in cities, delays can disrupt comfort and stability, “Even in London, the wait time for a clinician can be quite lengthy, unfortunately.” It’s in these waits, where minutes that feel like hours, that families often feel powerless. Unplanned hospital admissions follow, even when everyone knows the person wanted to stay at home.
Palliate steps into this gap, exploring whether carers can be trained to administer subcutaneous medications safely, compassionately, and with confidence.
Photography by Curated Lifestyle
Designing With, Not For: The Role of Lived Experience
To truly understand what families face at the end of life, the Palliate team turned to the people who know this landscape most intimately, our citizen longevity innovators, our Voice members. Their involvement brought depth, nuance and humanity to the work, guiding the research far beyond what could have been achieved through clinical expertise alone.
The process began with a series of honest, reflective conversations. Voice members spoke openly about the emotional and ethical complexities of administering medication to someone they love, a responsibility that carries its own weight, even when the practical steps are straightforward. Their reflections helped the team design an approach that felt realistic rather than idealised. As Dr Sunkersing explained, “When you know someone is dying, there are factors only lived experience can really give you, and that insight was incredibly valuable.”
It was during these conversations that something unexpected came up. Several Voice members asked a simple but important question, “After the person has passed away, what happens next? What support is there?” Palliate wasn’t designed to answer this, but the question stayed with the team. It pointed to a wider gap in how end-of-life care is often approached, with careful attention given up to the moment of death, and far less thought about what comes after. It was a reminder that caring doesn’t stop when the medication does, and that this part of the journey still needs more attention.
Learning Through Practice: What Hands-On Testing Revealed
The second phase of involvement brought Voice members into a hands-on setting at St Mary’s Hospital in London, Here, they tried three different styles of training, written instructions, written instructions and a paper “placemat,” and both the written instructions and placemat along with a video. This offered insights that could only emerge through real interaction with the materials. Two weeks later, they returned to repeat the task independently, giving the research team a clear sense of what felt intuitive, where confusion lingered, and what support might truly empower carers in real-life situations.
Rather than obstacles, the challenges they encountered became signposts helping to guide clearer instructions, safer design and more compassionate training.
Reflecting on this process, Dr Sunkersing said. “Overall it was received quite well and it definitely gave us the information we needed to refine and improve it.” And with equal honesty, he acknowledged the importance of what didn’t work.“ It wasn’t 100% flawless completion, which highlighted some challenges. Maybe we need more training, or instructions need to be more explicit.”
This openness strengthened the research, grounding it in the reality of caring rather than idealised scenarios. Voice members also spoke about what it meant to be part of the process. For Aurora, “watching our ideas take shape” was both inspiring and humbling, a sign that their contributions genuinely mattered. Warren echoed this, saying it was reassuring to see research that “places patient and carer voices at the heart.” Their reflections capture something essential, that through their curiosity, generosity and practical insight, Voice members have helped shape Palliate into a tool that is not only clinically grounded but deeply rooted in the lived realities of supporting someone at the end of life.
The time it took for someone in distress to receive symptom relief dropped from over 100 minutes to around 20, a shift families described as profoundly calming and empowering.
Early Signs of Real-World Change
A pre-pilot of Palliate has already revealed how transformative this approach could be. In most cases, 91% carers were able to give injections safely without a healthcare professional present, and their confidence averaged an impressive 8.73 out of 10. Crucially, the time it took for someone in distress to receive symptom relief dropped from over 100 minutes to around 20, a shift families described as profoundly calming and empowering. One carer captured it simply, “It made a massive difference, she trusted me. The alternative would have been delays and stress.” Together, these early results suggest that with the right support, carers can offer comfort precisely when it’s needed most.
What Comes Next?
The qualitative interview study has been accepted for publication, and analysis of the user-testing phase is underway. The team is now seeking funding to expand the project into community and hospice settings. Voice has been a vital part of this journey, as Dr Sunkersing acknowledges, “Voice helped us reach people beyond our usual networks, capturing a wide range of experiences, ages and backgrounds.”
The next phase is not only about scaling an intervention, it’s about deepening collaboration between researchers, clinicians, carers and communities.
Photography by Curated Lifestyle
Preparedness as a Gift
Palliate brings us closer to a part of life we rarely talk about, the practical and emotional work of caring for someone at home in their final days. It reminds us that preparedness isn’t clinical or cold, it’s a form of love. The simple ability to act, to ease someone’s discomfort, can become a gift, offered at a time when so much feels out of our control.
This work gently challenges the idea that only professionals can bring comfort, showing how lived experience can shape solutions that feel real, usable and human, grounded in the everyday reality of caring for someone you love.
It leaves us with questions that are both simple and profound, what if more families felt ready? What comfort could that unlock? What dignity could that restore?
Perhaps the future of end-of-life care won’t rest on new systems alone, but on who feels supported to help the people already sitting at the bedside, wanting to do just a little more.
You can read more about the project here.

 &
&